The hole-in-the-hand experiment that she is talking about is this: Hold your hand up to one eye. Hold a cardboard tube up to the other eye. If you have normal vision, you will fuse the images and it will appear that your hand has a hole in it. If you are completely suppressing, you will just see a cardboard tube OR your hand. If, like Bruce, you have ARC, you will see reality: a hand next to a cardboard tube.
When I read that passage, I thought to myself, "When I do the hole-in-the hand experiment, I see what Bruce sees.... And I feel like I still see a lot out of my deviated eye... Hmm... interesting. I must have that ARC business."
Before I discuss myself further, though, let me try to explain my understanding of ARC. Again, I could be misinformed, but this is how I have come to understand it.
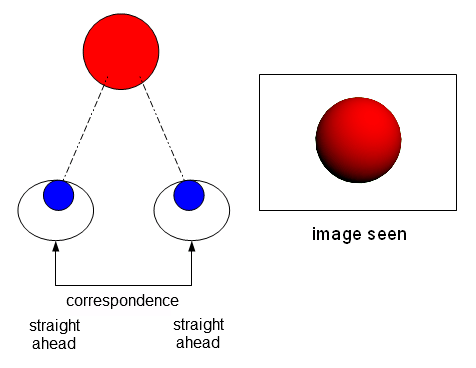
On the retina of each eye is an area called the fovea. It provides you with your clear, sharp central vision. In your brain, there is a LINK between these two foveas, and your brain operates under the assumption that the two foveas are ALWAYS pointing at the same place in space. In other words, the two foveas CORRESPOND to each other, and the brain fuses the image from each fovea into one stereoscopic image. Why does it fuse them together? Because, it is operating under the assumption that the two foveas always point to the same place in space.

This all works great when the two eyes are ACTUALLY pointing at the same thing, as in the image above. But what happens when one eye is strabismic and pointed at something else? Visual confusion or double vision results. Why?
Because the brain still believes that the two eyes point at the same place in space. Thus, it fuses the images together into a crazy mess.

Going through life with double vision and visual confusion is not very easy, though. So the brain usually adapts by suppressing the image from one eye, trying to create some semblance of normal vision.
The retinal link still remains intact.

There's a weirder, sneaker way that the brain can adapt, however. Break the retinal link! If the brain stops assuming that both eyes point at the same area of space, then the problem is solved. It adapts to the sad truth of reality: both eyes are NOT pointing at the same thing. Thus, each eye acts as an independent camera, with the images from both eyes being neatly pasted together in the middle.

This is ARC. The brain gives up on the notion that both eyes point at the same place in space. Instead of suppressing half of the visual field, it joins them together in the middle to create a panoramic view.
(I've read that ARC is much more common in esotropes, but I'm not sure how it works. Do they see a panorama? I'm not sure what they do...)
Anyway, back to myself. After reading that passage of Stereo Sue's book, I said "Okay, I have must have ARC. What an interesting factoid," and I didn't really think much of it. It wasn't until later, after researching it more, that I realized that it was not a good nor interesting thing. I read in Dr. Greenwald's book that Dr. Brock believed that ARC was incurable (though Dr. Greenwald himself did not believe this and had developed his own system for treating it). I also read that trying to convert ARC to NRC (normal retinal correspondence) can sometimes result in permanent double vision, and that some eye care professionals won't attempt it. And various other places, I just simply read that it was very hard to treat, with phrases like "exceedingly difficult" and "poor prognosis" being used.
At this point, I asked my optometrist and vision therapist if they thought I had ARC. Both of them didn't think that I did, and said that it was rare. My optometrist didn't think that I had it, but didn't really have the tools at the time to check if I had it or not.
So I said to myself, "I'll just figure it out myself." Here are my findings:
Josh's Findings
A report.
Hole in hand activity:
Result: Fail.
Camera flash test:
This classic ARC test involves flashing each eye with specially taped up camera flash.

-Hold it horizontally in front of one eye, stare at the piece of black tape in the middle. Flash.
-Hold it vertically in front of the other eye, stare at the piece of black tape in the middle. Flash.
-Close your eyes. Open your eyes. Look at a blank wall. Describe what you see.

When I do this test, I usually see one of the ARC versions. BUT, if I blink my eyes a lot, the two lines start moving toward each other into the NRC formation. What does that mean?!?! Fail? Pass?
Color Luster:
Wear red/green glass. Look at a light box. Try to mix the colors together. You fail if you see a half red light box, half green light box. My result: Mixed. I can see half red half green all day, but I can also make them mix a little if I squint and blink a lot.
Lid Glow:
Close one eye. Shine a penlight in your closed eye. Look at a black dot on the wall with your open eye. Try to make the black dot on the wall move into the glow you are receiving from your closed lid. Result: Pass... kind of. It's hard to do, but I can make it happen if I turn my head and blink a lot.
String test:
Wear red/green glasses. Hold a Brock string up to your nose. Fixate on a bead and make an X. If the GREEN string comes out of the RED eye, and the RED string comes out of the GREEN eye, you pass (crossed diplopia). Result: Passed with flying colors!
Bagolini Striated Lens test:
I won't go into detail about this test, but I got a weird result. I didn't get the ARC result, but I got uncrossed diplopia when I was supposed to have crossed diplopia (I think...). Result: Mystery.
Evidence for ARC:
I do a lot of things that one with ARC would do. When put on red/green glasses, relax my eyes, and look around the room, I see a half red half green room. I also feel that when doing fusion activities, I have to overcome the initial tendency to "paste" images from each eye together side by side. The first time I looked into the cheiroscope, I saw two totally separate images with no fusion. The same thing happened the first time I looked through a stereoscope, and the same thing happened when I first tried to do mirror overlap. Side by side images pasted together; panorama. I have also found it hard to gain even peripheral stereopsis, which is supposed to be "easy" (but this just changed today, see below).
Evidence against ARC:
I can also do a lot of things that one with ARC shouldn't be able to do. For example, I can make my eyes work as a team and play cards with antisuppression playing cards. I can see and play around with red/green tranaglyph slides. I can flat fuse a polarized vectogram into one image. I can do flat fusion stereoscope activities. And just today, I finally saw some depth on a polarized vectorgram! (but that's for another blog post).
Conclusion:
I believe have some ARC, but I am able to switch to NRC when doing vision therapy exercises that provide me with enough feedback (such as with anaglyphic activities and the Brock string).
I also believe that I have been self treating this ARC instinctively. When doing red/green anaglyphic activities, I often place objects that can only be seen by the RIGHT eye on the LEFT side, and objects seen by the LEFT eye on the RIGHT side. I then proceed to touch all over them with my hands to keep them "on." I have done this because it is "harder", and I now realize that it forces me to fuse the
whole visual area into one image, and reinforces it with motor feedback.
If the object that can only be seen by the RIGHT eye is placed on the RIGHT, and the object that can only be seen by the LEFT eye is placed on the LEFT, then it is possible for me to "paste" the images together, even when wearing red/green glasses. Thus, the activity can be rendered useless by a smart brain if you're not careful.
I certainly hope that my tendency for pasting images together in ARC fashion isn't an insurmountable obstacle for gaining binocular stereoscopic vision. I work very hard to do my vision therapy homework and to force my eyes to work as a team. And I am usually successful. But I still have that lingering fear... What if it never happens? What if my brain is just broken?